×
Il semble que vous utilisiez une version obsolète de internet explorer. Internet explorer n'est plus supporté par Microsoft depuis fin 2015. Nous vous invitons à utiliser un navigateur plus récent tel que Firefox, Google Chrome ou Microsoft Edge.
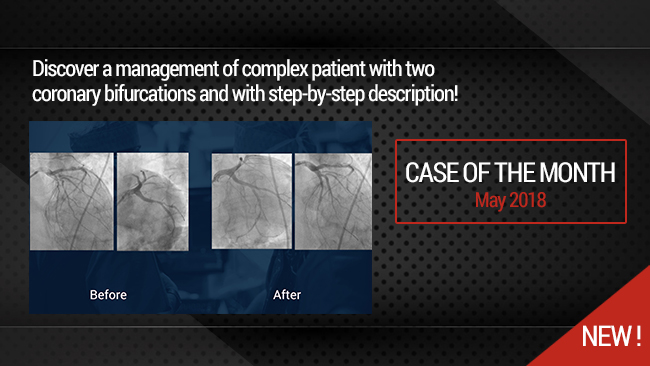
Simultaneous treatment of two coronary artery bifurcations in three vessels disease patient
Case of the Month: May 2018
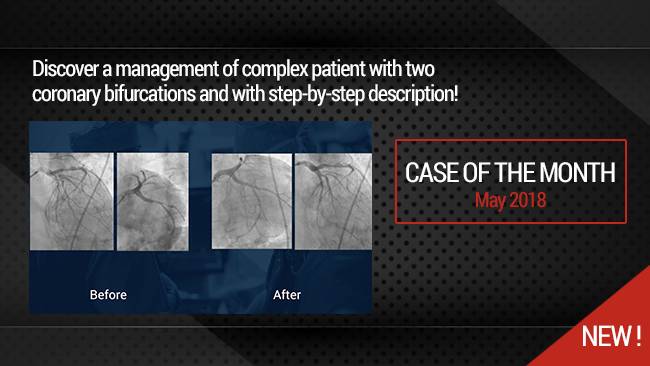
This didactic procedure concerns a 67 years old male with history of aortic valve infective endocarditis, presenting actually severe symptomatic aortic regurgitation with thoracic aortic aneuvrysm and three vessels coronary artery disease including two bifurcations lesions (LAD-Diag,Lcx-OM)
Since the patient is scheduled for Aortic surgery, All coronary lesions were treated in the same session using dedicated bifurcation stents Bioss Lim C with good final result .
Protocol
- Contrast volume: 330 ml Omnipaque (350mg)
- Procedure time: 70 min
- Exposure time: 21 mm
- Exposure: 18215,6 mGy
Learning points
- How to approach patients with multivessels coronary artery disease.
- Planning and approach complex bifurcation lesions.
- Concept of bifurcation dedicated stents.
- Two stents bifurcation PCI with dedicated stent (1.1.1) lesion (T stenting).
- Provisional bifurcation PCI with single dedicated stent (1.1.0) lesion.
- Multivessels coronary PCI (three lesions with 5 DES implentation) during the same session in selected patients.
Step-by-Step Procedure
- Right Arterial Femoral access 7F, EBU 7F guiding catheter.
- Wiring both LAD and 1st diagonal branch with Sion blue and Runthrough coronary PCI wires.
- Predilatation and stenting of the mid-LAD with Ultimaster 2.5x28mm DES.
- Predilatation of the 1st diagonal with 2.5x20mm balloon.
- Simultaneous positioning of LAD bifurcation stent (Bioss LimC: 3x3.75x16mm) and an Ultimaster 2.5x28mm stent in the 1st diagonal branch .
- Sequential stent deployment in the 1st diagonal, then in the proximal LAD.
- Optimization with POT-Kissing-rePOT sequence in the proximal LAD bifurcation.
- Wiring the Lcx and the OM branch.
- Direct stenting of the LCx to the OM branch with Bioss LIM C stent 2.75x3.25x24mm.
- POT technique for the LCx stent.
- JR4.0 6F guiding catheter in the RCA.
- Direct stenting with 3.5x33mm Ultimaster Terumo
- Access point closure with Perclose Device.
Biobliography
-
Percutaneous coronary intervention for coronary bifurcation disease: 11th consensus document from the European Bifurcation Club - Article
Authors:Jens Flensted Lassen, MD, PhD; Niels Ramsing Holm, MD
-
Regular Drug-Eluting Stent vs Dedicated Coronary Bifurcation BiOSS Expert Stent: Multicenter Open-Label Randomized Controlled POLBOS I Trial. - Article
Authors:Gil R, Bil , Džavík , Vassilev , Kern A, Formuszewicz R, Zalewska-Adamiec M, Dobrzycki s.
Publication:2015 May;31(5):671-8. doi: 10.1016/j.cjca.2014.12.024. Epub 2014 Dec 24
-
Regular drug-eluting stents versus the dedicated coronary bifurcation sirolimus-eluting BiOSS LIM® stent: the randomised, multicentre, open-label, controlled POLBOS II trial. - Article
Authors:Gil RJ, Bil J, Grundeken MJ, Kern A, Iñigo Garcia LA, Vassilev D, Pawłowski T, Formuszewicz R, Dobrzycki S, Wykrzykowska JJ, Serruys PW
Publication:2016 Dec 10;12(11):e1404-e1412. doi: 10.4244/EIJY15M11_11.
-
BiOSS LIM C: thin-strut cobalt-chromium version of the dedicated bifurcation stent. - Article
Authors:Gil RJ, Bil J, Kaczynski M, Milewski KP
Publication:2017 Apr;14(4):279-284. doi: 10.1080/17434440.2017.1318058. Epub 2017 Apr 19.
-
First-in-man study of dedicated bifurcation cobalt-chromium sirolimus-eluting stent BiOSS LIM C® - three-month results. - Article
Authors:Gil RJ, Bil J, Kern A, Pawłowski T.
Publication:2018;76(2):464-470. doi: 10.5603/KP.a2017.0226. Epub 2017 Dec 1.
-
Double bifurcation optimization stent system technique for left main stenosis. - Article
Authors:Vassilev D, Mateev H, Alexandrov A, Karamfiloff K, Gil RJ.
Publication: 2014 Dec;27(6):570-3. doi: 10.1111/joic.12155. Epub 2014 Sep 16.
Vidéos liées
Simultaneous treatment of two coronary artery bifurcations in three vessels disease patient
Dedicated coronary bifurcation stents - Case of the month: May 2018
Partager
Playlists liées

Our Cases of the Month
The case of the month is a new way for our users to watch, learn, and share with incathlab. They can watch a video that highlights an innovative case and uses excellent pedagogical techniques, lear...
Partager
{kind=link}