×
Il semble que vous utilisiez une version obsolète de internet explorer. Internet explorer n'est plus supporté par Microsoft depuis fin 2015. Nous vous invitons à utiliser un navigateur plus récent tel que Firefox, Google Chrome ou Microsoft Edge.
My Player placeholder
Crédit vidéo – Christian Vuolo – Synaps

Devenez membre d'Incathlab et bénéficiez d'un accès complet !

Vous devez être membre pour accéder aux vidéos Incathlab sans limitation. Inscrivez vous gratuitement en moins d'une minute et accédez à tous les services Incathlab ! Vous avez aussi la possibilité de vous connecter directement avec votre compte facebook ou twitter en cliquant sur login en haut à droite du site.
Inscription Connexion
Inscription Connexion
86813 vues
Case presentation:
Clinical Data:
- Man, 58 years, past smoking,
- 2011, september: ischemic stroke (right capsulo-lenticular location)
- Silent myocardial infarction, with a large inferior sequelae
- severe PAOD: infrarenal abdominal aorta occlusion, renal arteries stenosis, left subclavian artery occlusion
- 2011, september: recanalization and stenting of the left subclavian artery
Learning objectives:
- How to approach carotid arteries in case of severe abdominal aorta or ilio-femoral arteries disease?
- how to stage and how to schedule patients in case of multiple lesions?
- What are solutions for embolic distal protection and how to choose between the different devices available?
- Is there a place for IVUS and OCT in carotid artery stenting?
Procedural steps:
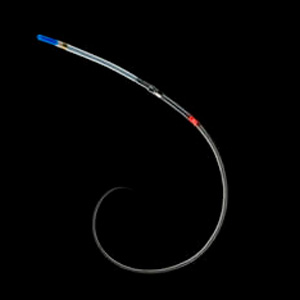
1. access:
- Right radial access, 6F, 10 cm Radiofocus, Terumo
- Canulation of the Right Common Carotid Artery with an angiographic catheter 5F, 100 cm, SIM 2 Super Torque, Cordis, advanced upon a 0,035" Radiofocus Terumo angled stiff guidewire M-type, 260 cm
- Exchange guidewire to with a 0,035" - 260 cm, Glidewire Advantage, Terumo
- Failure to advance the shuttle upon the Advantage Glidewire
- Repositioning of the SIM 2 Super Torque, Cordis, to position a 0,035" - 260 cm Extra Stiff Wire Guide, 0,035", Amplatz, Cook in the right common carotide artery
- Advance a 6F - 90 cm shuttle, Flexor, Cook, upon the Amplatz guidewire
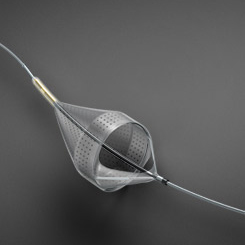
2. Distal protection device placement
- Anchoring of the shuttle with a V18 guidewire, Boston Scientific, placed in the external carotid artery
- Deploiement of a 7,2 x 23 mm Emboshield NAV system, Abbott, distal to the lesion
3. Performance of an OCT imaging:
- Pullback with an Imaging catheter, C7 DragonFly, St. Jude Medical advanced upon the guidewire of the Emboshield system
4. Stenting and postdilation:
- Retrieval of the V18 guidewire
- Deploiement of a Carotid stent System 7 - 9 x 30 mm Xact, Abbott
- Postdilation with a 5 x 20 mm Ultra Soft SV balloon, Boston Scientific
5. Control of the result by OCT
6. Retrieval of the Emboshield System
Date du tournage : 01/12/2011
Dernière mise à jour : 09/06/2021
Dernière mise à jour : 09/06/2021


{kind=link}
Multivascular patients management
Objectifs du cours Les patients Multivasculaires (plusieurs sites athéromateux), encore appelés polyvasculaires, représente 15% des patients explorés et prése...
Partager
{kind=link}
Suggestions
Left Carotid Artery Bypass Stenosis - Carotid artery stenting (Nextstent) with filter protection (Ru...
Clinique Louis Pasteur, Essey Les Nancy
Partager
Carotid Bifurcation Stenting for a Proximal ICA Stenosis
Department of Diagnostic & Interventional Radiology, Dortmund Teaching Hospital, Germany
Partager
Heavily Calcified Carotid Artery Stenosis
Management of Multivascular patients : Carotid + Coronary
Partager
Severe left internal carotid stenosis
Occluded Left vertebral artery supplied by left external carotid artery. Flow reversal for carotid p...
Partager
Very complex Internal Carotid Artery Stenting
Management of Multivascular patients : Carotid + Coronary
Partager
Stenting of a Right Carotid Bypass graft distal anastomosis with MOMA device protection
Louis Pasteur Clinic Essey les Nancy France
Partager