×
Il semble que vous utilisiez une version obsolète de internet explorer. Internet explorer n'est plus supporté par Microsoft depuis fin 2015. Nous vous invitons à utiliser un navigateur plus récent tel que Firefox, Google Chrome ou Microsoft Edge.
My Player placeholder
This didactic procedure concerns a 70 years old man, with multiple cardiovascular risk factors, presenting severe Left Limb Critical Ischemia with extensive gangrene in the II-III & IV toes.
He was treated by complete revascularization of both Anterior tibial artery (True to true lumen) & Posterior tibial artery recanalization, Good final angiographic result with acceptable Run off.
Educational objectives
- How to manage patients with Critical Limb ischemia & BTK vessels reocclusion.
- Optimal techniques to achieve complete revascularization in Critical Limb ischemia.
- How to minimize iodine contrast use during BTK revascularization procedures.
- Carboxy-dioxide angiography during BTK revascularization procedures.
- Drug Coated Balloon in BTK arteries.
Step-by-Step description
- Left CFA antegrade Access with 6F Sheath.
- Crossing Anterior tibial artery true lumen with 0.014 guidewire Command ES (Abbott).
- Crossing the Plantar Arch through the Dorsalis pedis artery using the Command ES guide wire & Ultraverse Balloon 2.0x40mm (BARD).
- Retrograde Crossing of the Posterior tibial artery till the proximal artery.
- Predilatation of the Anterior tibial artery & the plantar arch.
- Antegrade Crossing of the Posterior tibial artery with a second Command 0.014 guidewire (Abbott).
- Multilevel predilatation of the Posterior tivbial artery.
- Drug Coated balloon dilatation only for Anterior tibial artery.
- Second Balloon diltation of the Posterior tibial artery & the plantar arch.
- Final angiographic control with acceptable Run off & good patency of the ATA, PTA & plantar arch.
Biobliography
-
Peripheral Arterial Diseases (Diagnosis and Treatment of) ESC Clinical Practice Guidelines - Guidelines
Authors:Victor Aboyans Jean-Baptiste Ricco Marie-Louise E L Bartelink
Publication: European Heart Journal (2018) 39, 763–821
-
Lutonix® 014 DCB global Below the Knee Registry Study: interim 6-month outcomes. - Article
Authors: Thieme M, Lichtenberg M, Brodmann M, Cioppa A, Scheinert D.
Publication:doi: 10.23736/S0021-9509.18.10269-2. Epub 2018 Jan 23.
-
One Year Primary Patency of Infrapopliteal Angioplasty Using Drug- Eluting Balloons: Single Center Experience at King Hussein Medical Center. - Article
Authors:Haddad SE, Shishani JM, Qtaish I, Rawashdeh MA, Qtaishat BS.
Publication:doi: 10.4103/jcis.JCIS_34_17. eCollection 2017.
-
Drug-coated balloon angioplasty for the management of recurring infrapopliteal disease in diabetic patients with critical limb ischemia.ink title - Article
Authors:Palena LM, Diaz-Sandoval LJ, Gomez-Jaballera E, Peypoch-Perez O, Sultato E, Brigato C, Brocco E, Manzi M.
Publication: doi: 10.1016/j.carrev.2017.06.006. Epub 2017 Jun 20.
-
Automated Carbon Dioxide Angiography for the Evaluation and Endovascular Treatment of Diabetic Patients With Critical Limb Ischemia. - Article
Authors:Palena LM, Diaz-Sandoval LJ, Gomez-Jaballera E, Peypoch-Perez O, Sultato E, Brigato C, Brocco E, Manzi M.
Publication:doi: 10.1016/j.carrev.2017.06.006. Epub 2017 Jun 20.
Date du tournage : 23/03/2018
Dernière mise à jour : 11/05/2021
Dernière mise à jour : 11/05/2021


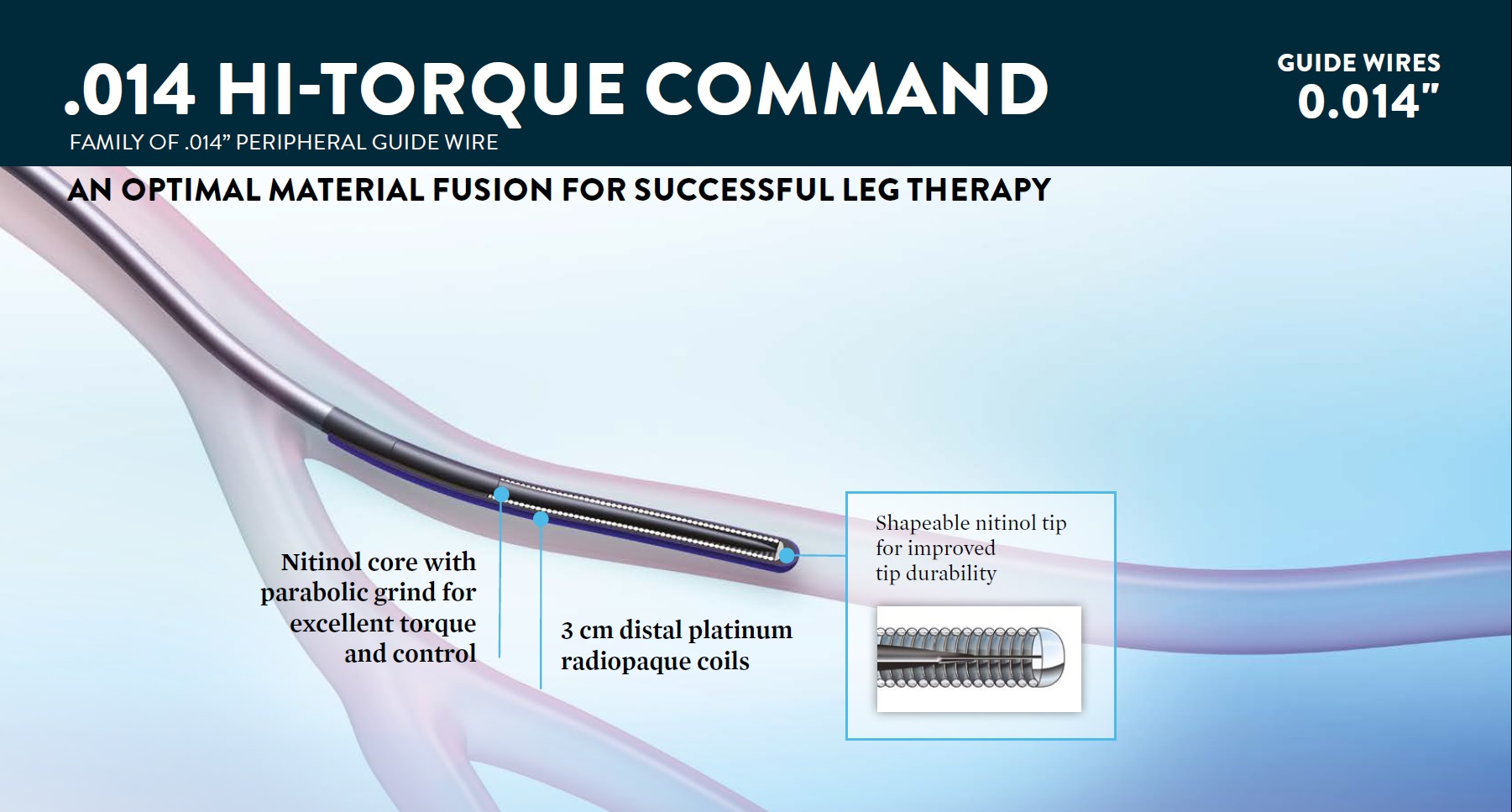
Hi-Torque Command Guide Wire / Abbott
Take Command of your peripheral cases

OptiRAY® / Guerbet
Optiray® contrast agent is lower osmolar, lower viscosity and nonionic.

Participer à la discussion
Suggestions

February 2017
Honolulu : Mercredi 15 février 2017 de 00h30 à 02h (GMT-10)
San Francisco : Mercredi 15 février 2017 de 02h30 à 04h (GMT-8)
New York : Mercredi 15 février 2017 de 05h30 à 07h (GMT-5)
Buenos Aires : Mercredi 15 février 2017 de 07h30 à 09h (GMT-3)
London / Dublin : Mercredi 15 février 2017 de 10h30 à 12h (GMT)
Paris / Berlin : Mercredi 15 février 2017 de 11h30 à 13h (GMT+1)
Istanbul : Mercredi 15 février 2017 de 12h30 à 14h (GMT+2)
Moscou / Dubaï : Mercredi 15 février 2017 de 14h30 à 16h (GMT+4)
Bangkok : Mercredi 15 février 2017 de 17h30 à 19h (GMT+7)
Shanghai : Mercredi 15 février 2017 de 18h30 à 20h (GMT+8)
Tokyo : Mercredi 15 février 2017 de 19h30 à 21h (GMT+9)
Sydney : Mercredi 15 février 2017 de 20h30 à 22h (GMT+10)
Wellington : Mercredi 15 février 2017 de 22h30 à 00h (GMT+12)
San Francisco : Mercredi 15 février 2017 de 02h30 à 04h (GMT-8)
New York : Mercredi 15 février 2017 de 05h30 à 07h (GMT-5)
Buenos Aires : Mercredi 15 février 2017 de 07h30 à 09h (GMT-3)
London / Dublin : Mercredi 15 février 2017 de 10h30 à 12h (GMT)
Paris / Berlin : Mercredi 15 février 2017 de 11h30 à 13h (GMT+1)
Istanbul : Mercredi 15 février 2017 de 12h30 à 14h (GMT+2)
Moscou / Dubaï : Mercredi 15 février 2017 de 14h30 à 16h (GMT+4)
Bangkok : Mercredi 15 février 2017 de 17h30 à 19h (GMT+7)
Shanghai : Mercredi 15 février 2017 de 18h30 à 20h (GMT+8)
Tokyo : Mercredi 15 février 2017 de 19h30 à 21h (GMT+9)
Sydney : Mercredi 15 février 2017 de 20h30 à 22h (GMT+10)
Wellington : Mercredi 15 février 2017 de 22h30 à 00h (GMT+12)
New frontiers of complex SFA angioplasties
Conquering the Complex lesions with step-by-step approach
Partager

{kind=link}
{kind=link}
CLIC 2019 SESSION V: SURGERY VERSUS ENDO FOR COMPLICATIONS MANAGEMENT
Critical Limb Ischemia Course
Partager
Mangesh T. Very well done BTK & BTA Tibial Arterial DCB Plasty with excellent foot perfusion results.
But Why not use “Phoenix Hybrid (Rotational & Directional) Atherectomy device for debulking heavily calcified distal PTA & dorsal Foot arch or at least Shockwave Lithoplasty balloons to beat Calcium??
v22e V. Excelent case
v22e V. Thanks